CLOSTRIDIA: SPOREFORMING ANAEROBIC BACILLI
AUTHOR: Ayesha Rasheed (Microbiologist)
Qurat ul Ain (Microbiologist)
Farida Bibi (Microbiologist)
Introduction:
The clostridia are large, Gram – positive bacteria which are fermentative, catalase – negative and oxidase negative, and require enriched media for growth. They are straight or slightly curved rods and the majority are motile by flagella which are peritrichous. Clostridium species produce endospores which usually cause bulging of mother cells. The size, shape and location of endospores can be used for species differentiation. Although most pathogenic clostridial species are strict anaerobes, some are com paratively aerotolerant. Clostridia occur worldwide and particular species may be associated with defined geographical regions.
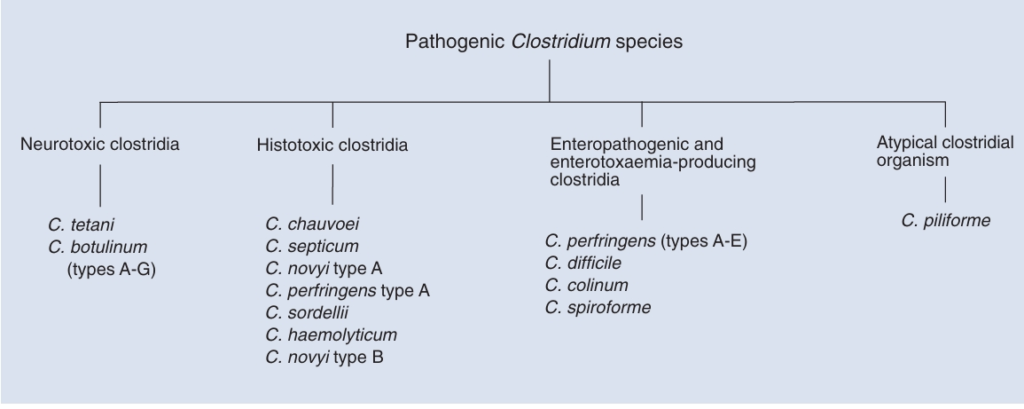
Although more than 100 clostridial species are recognized, less than 20 are pathogenic. These pathogenic species can be grouped in three categories, based on toxin activity and tissues affected. Clostridium tetani and C. botulinum, the neurotoxic clostridia, affect neuromuscular function without inducing observable tissue damage. In contrast, histotoxic clostridia produce relatively localized lesions in tissues such as muscle and liver and may subsequently cause toxemia. Clostridium perfringens types A to E, important members of the third category, and produce inflammatory lesions in the gastrointestinal tract along with enterotoxaemia. Clostridium difficile is an emerging enteric pathogen of animals and is a significant nosocomial pathogen of humans. Clostridium spiroforme causes diarrhea in rabbits and C. colinum is an intestinal pathogen of fowl. Clostridium piliforme, which causes hepatic necrosis in foals, is an atypical member of the clostridia and does not have characteristics that permit its inclusion in any of the three categories described.
Of the anaerobes that infect humans, the clostridia are the most widely studied. They are involved in a variety of human diseases, the most important of which are gas gangrene, tetanus, botulism, pseudomembranous colitis and food poisoning. In most cases, clostridia are opportunistic pathogens; that is, one or more species establishes a nidus of infection in a particular site in a compromised host. All pathogenic clostridial species produce protein exotoxins (such as botulinum and tetanus toxins) that play an important role in pathogenesis.
Usual habitat:
Clostridia are saprophytes which are found in soil, freshwater or marine sediments with suitably low redox potentials. They constitute part of the normal intestinal flora and some may be sequestered as endospores in muscle or liver. Sequestered endospores, if activated, may produce disease.
Clinical conditions caused by neurotoxic clostridia:
The neurotoxic clostridia, C. tetani and C. botulinum, produce their effects by elaborating potent neurotoxins. The neurotoxin of C. tetani is produced by organ isms replicating locally in damaged tissues. Absorbed toxin exerts its effect on synaptic junctions remote from the site of toxin production. The neurotoxin of C. botulinum is usually produced by organisms replicating in decaying organic matter or in the anaerobic conditions in contaminated cans of meat or vegetables. When absorbed from the gastrointestinal tract into the bloodstream, the toxin affects the functioning of neuromuscular junctions. The toxins of both C. tetani and C. botulinum are similar in structure and function. The differing clinical signs observed in each disease can be explained by the differing sites of action of the toxins produced by each organism.
Clinical conditions caused by histotoxic clostridia:
Histotoxic clostridia produce a variety of lesions in domestic animals. The exotoxins elaborated by replicating bacteria induce both local tissue necrosis and systemic effects which may be lethal. Some histotoxic clostridia are present in the tissues as latent spores which can germinate and produce specific clinical diseases. These include C. chauvoei and occasionally C. septicum in muscle tissue, and C. novyi type B and C. haemolyticum in the liver. Histotoxic clostridia introduced into wounds, often as mixed infections, can cause malignant oedema and gas gangrene. The clostridial species involved include C. chauvoei, C. septicum, C. novyi type A, C. perfringens type A and, occasionally, C. sordellii. The abomasitis caused by C. septicum in sheep (braxy) is an example of a local histotoxic effect.
Enteropathogenic and enterotoxaemia producing clostridia:
Clostridia that produce enterotoxaemia and enteropathy replicate in the intestinal tract and elaborate toxins that produce both localized and generalized effects. Pathogenic strains of these clostridia may be present in the intestinal flora of animals but only produce disease in defined circumstances.
Tetanus and Clostridium tetani:
Clinical Manifestations:
Tetanus is a severe disease caused by the toxin of C tetani (Fig.). This organism grows in a wound and secretes a toxin that invades systemically and causes muscle spasms. The initial symptom is cramping and twitching of muscles around a wound. The patient usually has no fever but sweats profusely and begins to experience pain, especially in the area of the wound and around the neck and jaw muscles (trismus). Portions of the body may become extremely rigid, and opisthotonos (a spasm in which the head and heels are bent backward and the body bowed forward) is common. Complications include fractures, bowel impaction, intramuscular hematoma, muscle ruptures, and pulmonary, renal, and cardiac problems.
Figure
Pathogenesis of tetanus caused by C tetani.
Structure and Classification:
C tetani is an anaerobic gram-positive rod that forms terminal spores, giving it a characteristic tennis racquet appearance. Some strains do not sporulate readily, and spores may not appear until the third or fourth day of culture. Most strains are motile with peritrichous flagella; colonies often swarm on agar plates, but some strains are non-flagellated and non-motile. The presence of C tetani should be suspected on isolation of a swarming rod that produces indole and has terminal spherical spores, but does not produce acid from glucose. Toxigenic C tetani contains a plasmid that produces a toxin called tetanospasmin, but nontoxigenic strains also exist. Tetanospasmin is responsible for the infamous toxemia called tetanus. The two animal species most susceptible to this toxemia are horses and humans.
Pathogenesis:
As with all clostridial wound infections, the initial event in tetanus is trauma to host tissue, followed by accidental contamination of the wound with C tetani (Fig.). Tissue damage is needed to lower the oxidation-reduction potential and provide an environment suitable for anaerobic growth. Once growth is initiated, the organism itself is not invasive and remains confined to the necrotic tissue, where the vegetative cells of C tetani elaborate the lethal toxin. The incubation period from the time of wounding to the appearance of symptoms varies from a few days to several weeks, depending on the infectious dose and the site of the wound (the more peripheral the wound, the longer the incubation time).
Tetanus can be initiated in two different ways, resulting in either generalized or local tetanus. In generalized tetanus (also called descending tetanus), all of the toxin cannot be absorbed by local nerve endings; therefore, it passes into the blood and lymph with subsequent absorption by motor nerves. The most susceptible centers are the head and neck; the first symptom is usually trismus (lockjaw), with muscle spasms descending from the neck to the trunk and limbs. As the disease progresses, the spasms increase in severity, becoming very painful and exhausting. During spasms, the upper airway can become obstructed, resulting in respiratory failure. Spasms often are initiated by environmental stimuli that may be as insignificant as the flash of a light or the sound of a footstep. In the localized form of tetanus (also called ascending tetanus), toxins travel along the neural route (peripheral nerves), causing a disease confined to the extremities and seen most often in inadequately immunized persons. Localized tetanus may last for months but usually resolves spontaneously. Another unusual form of tetanus is called cephalic tetanus which results from head wounds and affects the face, most commonly the muscles innervated by lower cranial nerves. Curiously, cephalic tetanus can occur in fully immunized persons; the outcome is typically poor, but mild cases (often associated with otitis media) have more favorable outcomes. Neonatal tetanus is seen in newborns when the mother lacks immunity and the umbilical stump becomes contaminated with C tetani spores.
C tetani actually produces two toxins: tetanolysin, a hemolysin that is inactivated by cholesterol and has no role in pathogenesis, and tetanospasmin, a spasmogenic toxin responsible for the classical symptoms of the disease.
The actions of tetanospasmin are complex and involve three components of the nervous system: central motor control, autonomic function, and the neuromuscular junction. Toxin enters the nervous system primarily through the neuromuscular junction of alpha motor neurons. The toxin is then transported to the other neurons, most importantly presynaptic inhibitory cells, where it is no longer accessible to be neutralized by antitoxin. (This retrograde transport to the central nervous system is similar to that utilized by some viruses, such as herpes virus and rabies.) The toxin also spreads hematogenously, but it still must enter the central nervous system via retrograde transport from peripheral neuronal processes. Once the toxin gains access to inhibitory neurons, it blocks the release of the neurotransmitters glycine and gamma-aminobutyric acid. The absence of this inhibition permits the simultaneous spasms of both agonist and antagonist muscles, producing muscle rigidity and convulsions. Tetanospasmin also acts on the autonomic nervous system and is associated with elevated plasma catecholamine levels; respiratory failure is a frequent complication of the disease. Peripherally, there is a failure of transmission at the neuromuscular junction, involving defective release of acetylcholine in a manner similar to that seen with C botulinum. Tetanospasmin may be as potent as the toxin of C botulinum; as little as 130 µg constitutes a lethal dose for humans. In untreated tetanus, the fatality rate is 90% for the newborn and 40% for adults. However, with aggressive hospital care, these fatality rates can be substantially reduced. The ultimate cause of death is usually pulmonary or cardiac failure.
Host Defenses:
Although there are scattered reports that tetanus antibodies can be acquired by natural, presumably enteric, infection with C tetani, innate immunity to tetanus toxin does not typically exist. In addition, one or more episodes of tetanus do not produce immunity to future attacks. The reason for the lack of immune response may be twofold: the toxin is potent, and the amount released may be too small to trigger immune mechanisms but still be enough to cause symptoms and, because the toxin binds firmly to neural tissue, it may not interact effectively with the immune system.
Epidemiology:
C tetani can be isolated from the soil in almost every environment throughout the world. The organism can be found in the gastrointestinal flora of humans, horses, and other animals. Isolation of C tetani from the intestinal flora of horses, coupled with the high frequency of equine tetanus, led to the erroneous assumption that the horse was the animal reservoir of C tetani.
Generalized outbreaks of tetanus do not occur, but certain populations can be considered at risk. Historically, wounded soldiers have had a high incidence of tetanus, but this phenomenon declined with widespread use of immunizations. Umbilical tetanus (tetanus neonatorum) usually is a generalized, fulminating, fatal disease that occurs with the neonates of unimmunized mothers who have given birth under unsanitary conditions. In the United States, intravenous drug abusers have become another population with an increasing incidence of clinical tetanus. One million cases of tetanus occur annually in the world. Tetanus is rare in most developed countries. The United States has about one case per million per year, most often seen in the elderly with declining immune status due to failure to receive timely tetanus booster vaccinations. In some less developed countries, tetanus is still one of the ten leading causes of death, and neonatal tetanus accounts for approximately one-half of the cases worldwide. In less developed countries, approximate mortality rates remain 85% for neonatal tetanus and 50% for non-neonatal tetanus. This is an unfortunate situation because with adequate immunization, tetanus is a completely preventable disease.
Diagnosis:
Diagnosis of tetanus is obvious in advanced cases; however, successful treatment depends on early diagnosis before a lethal amount of toxin becomes fixed to neural tissue. The patient should be treated on a clinical basis without waiting for laboratory data. C tetani can be recovered from the wound in only about one-third of the cases, and a wound is not even evident in 10–20% of cases. It is important for the clinician to be aware that toxigenic strains of C tetani can grow actively in the wound of an immunized person, but the presence of antitoxin antibodies prevents initiation of tetanus. Also, because tetanus is commonly found in the soil, the mere presence of tetanus in a wound does not imply that the organism is actively replicating and secreting toxin.
Numerous syndromes, including rabies and meningitis, have symptoms similar to those of tetanus and must be considered in the differential diagnosis. Ingestion of strychnine (found in rat poison) can cause symptoms that closely resemble those of generalized tetanus. Trismus can occur in encephalitis, phenothiazine reactions, and diseases involving the jaw.
Control:
Injections of tetanus toxoid are prophylactic. Currently, booster doses are recommended only every 10 years by the CDC. More frequent boosters are unnecessary and may cause local reactions resembling the Arthus phenomenon or a delayed hypersensitivity reaction. It has been noted that, because of their immunodeficiency state, AIDS patients may not respond to prophylactic injections of tetanus toxoid. An antibody titer above 0.01 international units (IU) per ml is usually considered protective. Human tetanus immunoglobulin (HTIG) in a dose of 250 IU intramuscularly should be considered for those with questionable immune status.
Treatment of diagnosed tetanus has a number of aspects. The offending organism must be removed by local debridement, after the patient’s spasms are controlled by benzodiazepines. Penicillin or metronidazole is usually administered to kill the bacteria, but may not be a necessary adjunct in therapy. Although penicillin has been historically considered to be the drug of choice, it has been speculated that penicillin could have an adverse effect by acting synergistically with tetanospasmin. Metronidazole is currently recommended, and there is some evidence that it is associated with an improved prognosis. HTIG is injected intramuscularly: dosage recommendations vary from 500 IU in a single intramuscular injection to 3000–6000 IU injected intramuscularly in several sites. Supportive measures, such as respiratory assistance and intravenous fluids, are often critical to patient survival. Recommended treatment includes benzodiazepines, such as diazepam (Valium). Analgesics that will not cause respiratory depression should be used, and include codeine, meperidine (Demerol), and morphine. Adequate nutritional support should be provided and should consider that the patient’s nutritional needs are extraordinarily great.
In cases of clean, minor wounds, tetanus toxoid should be administered only if the patient has not had a booster dose within the past 10 years. For more serious wounds, toxoid should be administered if the patient has not had a booster dose within the past 5 years. All patients who have a reasonable potential for contracting tetanus should receive injections of tetanus immunoglobulin, including those recovering from diagnosed cases of tetanus.
References:
Akbulut, D., Grant, K.A. and McLauchlin, J. (2005). Improvement in laboratory diagnosis of wound botulism and tetanus among injecting illicit – drug users by use of real – time PCR assays for neurotoxin gene fragments. Journal of Clinical Microbiology, 43, 4342 – 4348.
AOAC International (2001). AOAC Official Method 977.26 (Sec. 17.7.01) Clostridium botulinum and its toxins in foods. Official Methods of Analysis, 17th Edition. AOAC International, Gaithersburg, MD.
B å verud, V. (2004). Clostridium difficile diarrhea: infection control in horses. Veterinary Clinics of North America, Equine Practice, 20, 615 – 630.
Berry, A.P. and Levett, P.N. (1986). Chronic diarrhea in dogs associated with Clostridium difficile infection. Veterinary Record, 118, 102 – 103.
Borchers , A. , Magdesian , K.G. , Halland , S. , Pusterla , N. and Wilson , W. D. ( 2006 ). Successful treatment and polymerase chain reaction (PCR) confirmation of Tyzzer’s disease in a foal and clinical and pathologic characteristics of six additional foals (1986 – 2005). Journal of Veterinary Internal Medicine, 20, 1212 – 1218.
Borriello, S.P. and Carman, R.J. (1983). Association of an iota – like toxin and Clostridium spiroforme with both spontaneous and antibiotic – associated diarrhea and colitis in rabbits. Journal of Clinical Microbiology, 1, 414 – 418.
Buxton, D., Linklater, K.A. and Dyson, D.A. (1978). Pulpy kidney disease and its diagnosis by histological examination. Veterinary Record, 102, 241.
Cai, S.W. and Singh, B.R. (2007). Botulism diagnostics: from clinical symptoms to in vitro assays. Critical Reviews in Microbiology, 33, 109 – 125.
Anand A, Glatt AE. Clostridium difficile infection associated with antineoplastic chemotherapy: a review. Clin Infect Dis. 1993; 17:109.
Bartlett JG. Clostridium difficile: History of its role as an enteric pathogen and the current state of knowledge about the organism. Clin Infect Dis. 1994; 18:S265.
Bongaerts GPA, Lyerly DM. Role of toxins A and B in the pathogenesis of Clostridium difficile disease. Microbial Pathogenesis. 1994; 17:1.
Bleck TP. Tetanus: pathophysiology, management, and prophylaxis. Disease-A-Month. 1991; 37:545.
Coffield JA, Considine RV, Simpson LL. Clostridial neurotoxins in the age of molecular medicine. Trends in Microbiology. 1994; 67:67.